

Watch More! Unlock the full videos with a FREE trial
Included In This Lesson
Study Tools
Access More! View the full outline and transcript with a FREE trial
Outline
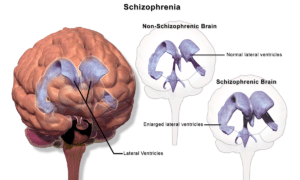
Pathophysiology
Schizophrenia is a serious mental disorder that affects how a person thinks, feels and behaves. Patients often have difficulty distinguishing between reality and imagination and have difficulty communicating with others. Schizophrenia tends to run in families, but most frequently appears to be related to an imbalance of neurotransmitters (dopamine, glutamate and serotonin) that change the way the brain reacts to stimuli. Patients are not normally violent but may react defensively to even the most well-intended gestures or stimuli.
Etiology
Diagnostic Criteria:
The patient must have experienced at least two of the following symptoms, one of which must be a positive symptom.
- Positive symptoms
- Delusions
- Hallucinations
- Disorganized speech
- Disorganized (or catatonic) behavior
- Negative symptoms
- Flat affect
- Decrease in emotional range
- Loss of interest in activities
- Reduced speaking
Symptoms must be present for at least 6 months with at least one month of active symptoms. Symptoms are not related to substance use/abuse or any other medical condition.
Desired Outcome
Patient will communicate effectively. Patient will demonstrate reality-based thought processes. Patient will demonstrate ability to distinguish between reality and hallucinations.
Schizophrenia Nursing Care Plan
Subjective Data:
- Hallucinations
- Feeling of being watched (paranoia)
- Change in personality
- Inability to sleep
- Inability to concentrate
- Feelings of indifference
Objective Data:
- Awkward body positioning
- Decreased or impaired speech
- Decline in academic or work performance
- Inappropriate behavior
- Extreme preoccupation with religion or the occult
- Flat affect
- Unprovoked outbursts or uninhibited actions
- Tense, anxious or erratic movements
- Wandering
Nursing Interventions and Rationales
- Obtain history and assess patient for hostile or self-destructive behaviors
Determine risk of harm to patient or others and what precautions may be required. Stress response often triggers hallucinations.
- Provide encouragement in a non-judgemental, compassionate way, understanding that symptoms are real to patient
Develop trust between patient and nurse to improve effectiveness of interventions and cooperation.
- Encourage patient to communicate (verbal, drawing, written) how hallucinations make them feel
Helps understand and anticipate behaviors and help identify stressors such as fear or helplessness. Reduce anxiety.
- Ask if hallucinations are instructing them to harm themselves or others. Provide safety for patient and others per facility protocol if needed.
Patients may be inclined to obey commands given by hallucinations that instruct them to harm themselves or others. Notify security or police if necessary.
Follow your facility’s specific protocol regarding supervision, restraint, and documentation.
- Provide redirection for inappropriate behaviors, maintain boundaries and guidelines.
Avoids need for intervention and exacerbated behaviors. Redirecting patient helps remove the focus from the current perceived threat to a more positive activity.
Boundaries and guidelines should be held consistently among caregivers to prevent splitting (turning one caregiver against another).
- Encourage reality-based activities (music, art, playing cards, etc.)
Help redirect patient to acceptable activities and behaviors and reduce the risk of hallucinatory distractions.
- Explain all procedures slowly and carefully before beginning
Reduces paranoia and encourages cooperation. Patients are less likely to feel “tricked” if they understand what is happening to them. Even taking a blood pressure can be frightening if not fully explained first.
- Avoid using large gestures or touching the patient except when necessary
Patient’s distortion of reality may interpret the touch or gesture as an aggressive or threatening action.
- Gently reorient patient as necessary
Reorienting patient helps them differentiate between reality and hallucination.
- Avoid arguing with a patient regarding delusions or hallucinations
If reorienting is initially ineffective, avoid persistent attempts or arguing as it can agitate the patient or cause feelings of isolation.
Never confirm a delusion or hallucination (“I see Jesus, too!”) – this can exacerbate agitation or confusion.
- Teach patient coping skills to help manage hallucinations or delusions
- Exercise
- Singing / listening to music
- Writing
- Drawing
- Talking with someone they trust
Help patient learn how to cope with and manage symptoms to improve daily functioning and behaviors.
- As symptoms improve, allow patient to make small decisions such as what to eat, wear or choice of activities
Allows patient to feel that they have more control of themself and their care. Promotes independence.
- Administer medication appropriately
Routine medications may be given to help improve symptoms.
- Atypical antipsychotics
IM medications may be given PRN for acute exacerbations.
- Diphenhydramine
- Haloperidol
- Lorazepam
References
View the FULL Outline
When you start a FREE trial you gain access to the full outline as well as:
- SIMCLEX (NCLEX Simulator)
- 6,500+ Practice NCLEX Questions
- 2,000+ HD Videos
- 300+ Nursing Cheatsheets
“Would suggest to all nursing students . . . Guaranteed to ease the stress!”







